Women's Health
Reproductive healthcare appointment scheduling that provides an open line of communication between patients and providers.
The Women's Health application gives users flexibility and autonomy to choose a reproductive healthcare provider based on their needs including but not limited to gender, race, insurance, price, health concerns, reviews, and previous client demographics providers have experience working with. Users can request appointments with specific details about health concerns to address in the appointment to avoid missing information and to alleviate any discomfort in speaking about sensitive topics. Healthcare providers can then accept/decline appointment requests, view comments/details provided by patients to be discussed in appointments and are shown literary research regarding related topics. Patients and providers can communicate after appointments to discuss aftercare plans as well.
Roles
- UX Designer
- UX Researcher
- Product Designer
Deliverables
- Behavioral archetype
- One-on-one interviews
- Journey map
- Design strategy
- Low-fidelity prototype
Specifications
- Class: Behavioral Science and UX
- Duration: 10 weeks
- Tools: Figma and Canva
Problem Statement
The issue being addressed here is gender bias in reproductive healthcare in the United States. This is an important behavior change area because many women, especially women of color and/or women from underprivileged areas, struggle to receive the reproductive healthcare they need due to stigmatization/bias from healthcare providers.
Target Audience
The target audience for this project is women and people seeking reproductive healthcare services living in the United States. Another audience being targeted here is reproductive healthcare providers themselves looking to strengthen client relationships and build new ones.
User Research
The primary objective of this research is to understand the experiences and pain points of women when visiting their reproductive healthcare providers and what would help ease those issues. The following questions will help guide one-on-one interviews with participants:
- How can healthcare providers create more trusting relationships/environments for patients?
- How can healthcare providers give more information/resources beyond pregnancy related issues to patients? How can they create more personalized/comfortable experiences? (e.g. many women feel discomfort discussing sexual health because they are not probed with questions related to topics other than pregnancy)
- How can healthcare providers remove their biases when their patients are from a marginalized background?
- How can healthcare policies and providers be more inclusive and understanding of patients from all demographics?
Emerging Themes
Goals, Mental Models, and Self-Agency: People are seeking familiarity when searching for a healthcare provider. They believe they will be better understood when their healthcare provider is similar to them in some way (age, gender, culture, ethnicity, etc.).
- People value being able to filter through doctors using preferences to find one that matches their age/race/sexual identity.
- They value reviews and ratings. This gives a sense of self-agency.
- The main goal/objective when seeking healthcare providers is feeling heard and understood by doctors.
- People tend to gravitate towards healthcare providers who are similar to them in order to decrease the perceived bias that has historically existed in patient/doctor relationships.
Communication and Power Dynamics: Power dynamics between healthcare providers and patients can sometimes create a negative effect on trust and comfortability on the patient’s end. Patients feel hopeless or unheard by doctors when their systems are dismissed or ignored. Clear and equitable communication was a common trait mentioned by participants when asked “what does good communication look like?”
- Participants talked about having to do their own research about certain advice/suggestions given by their healthcare providers to ensure they were given accurate information. In some cases, they were not given adequate or correct information.
- Participants mentioned wanting to be able to have open conversations and reasoning behind decisions being made by doctors about their health goals.
Coping and Power Dynamics: People will avoid doctors who are not like them or who they perceive to be different or difficult to connect to. People will mentally prepare beforehand for appointments in which they anticipate discrimination. People will be uncomfortable during their visit and answer questions they do not want to.
- Participants spoke about having a preventable and easily curable diagnosis but will avoid the doctor and live with the pain/discomfort.
Frameworks for Understanding
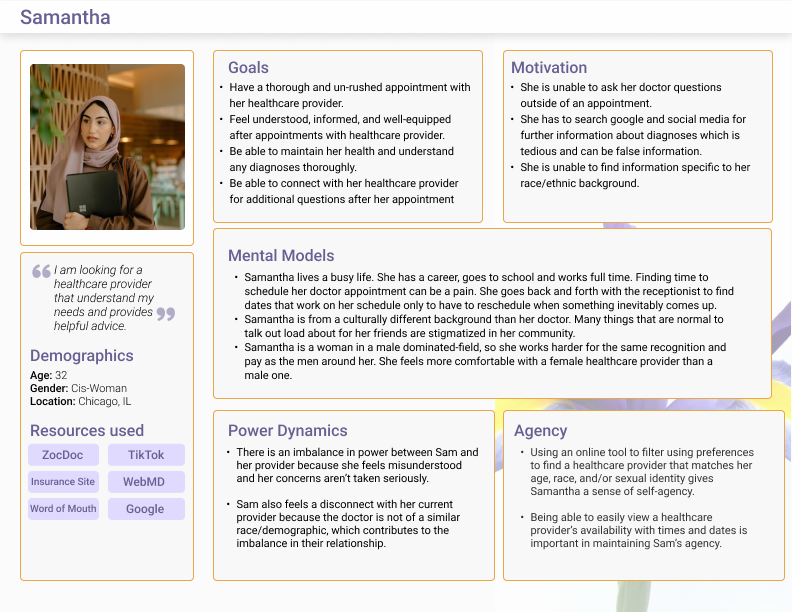
Behavioral Archetype
The following user persona was created based off common themes found from user interviews. Our journey map guides this user through all of the stages of scheduling, executing, and processing appointments with reproductive healthcare providers in order to reach the goals listed.
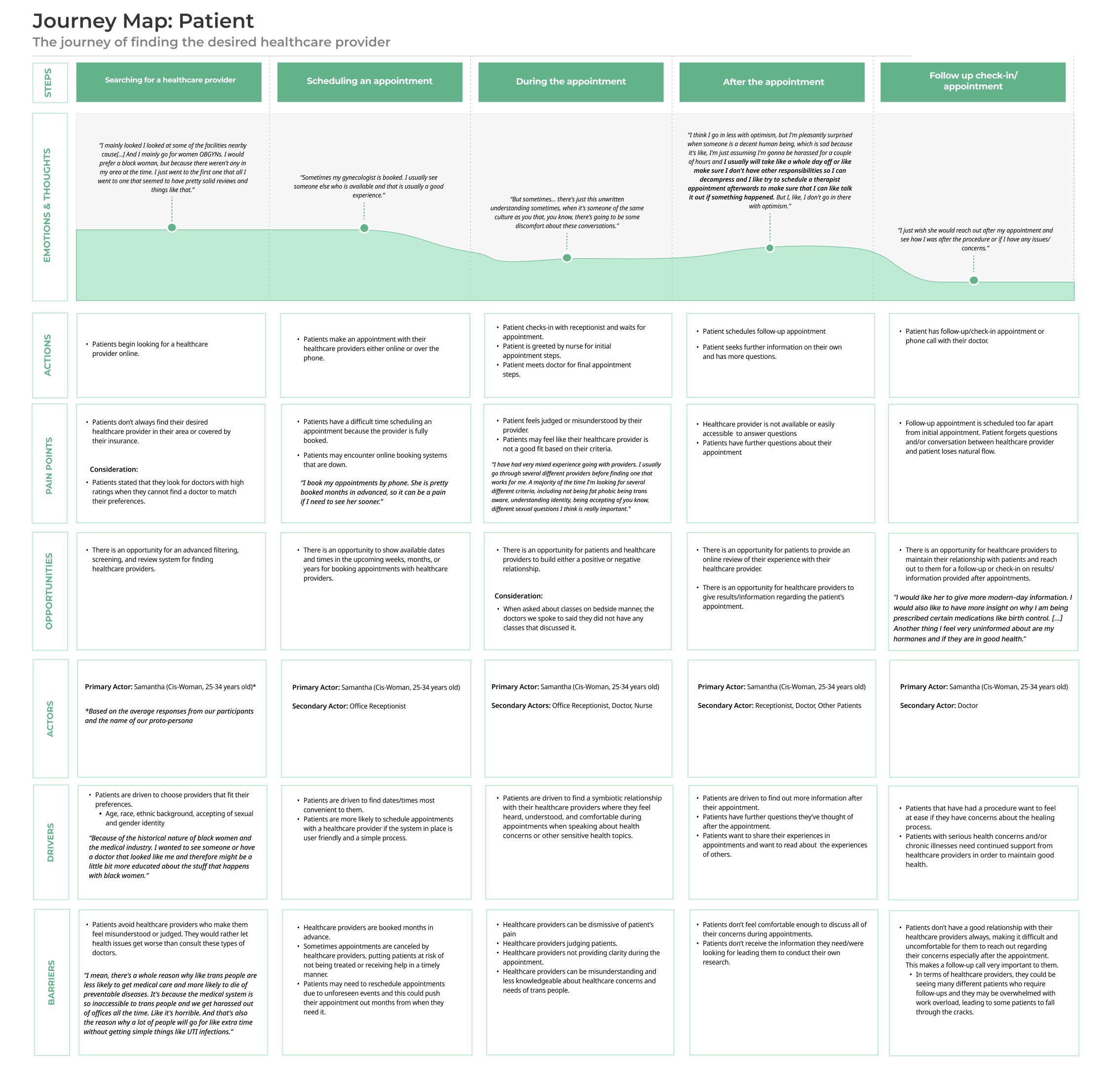
Journey Map
Outlined in each stage of the journey are the user's emotions, thoughts, actions, pain points, opportunities, drivers, and barriers that influence reaching the end goal of finding their desired healthcare provider. Our journey map displays the following milestones users will experience before, during, and after reproductive healthcare appointments:
- Searching for a healthcare provider
- Scheduling an appointment
- During the appointment
- After the appointment
- Follow-up and aftercare plan
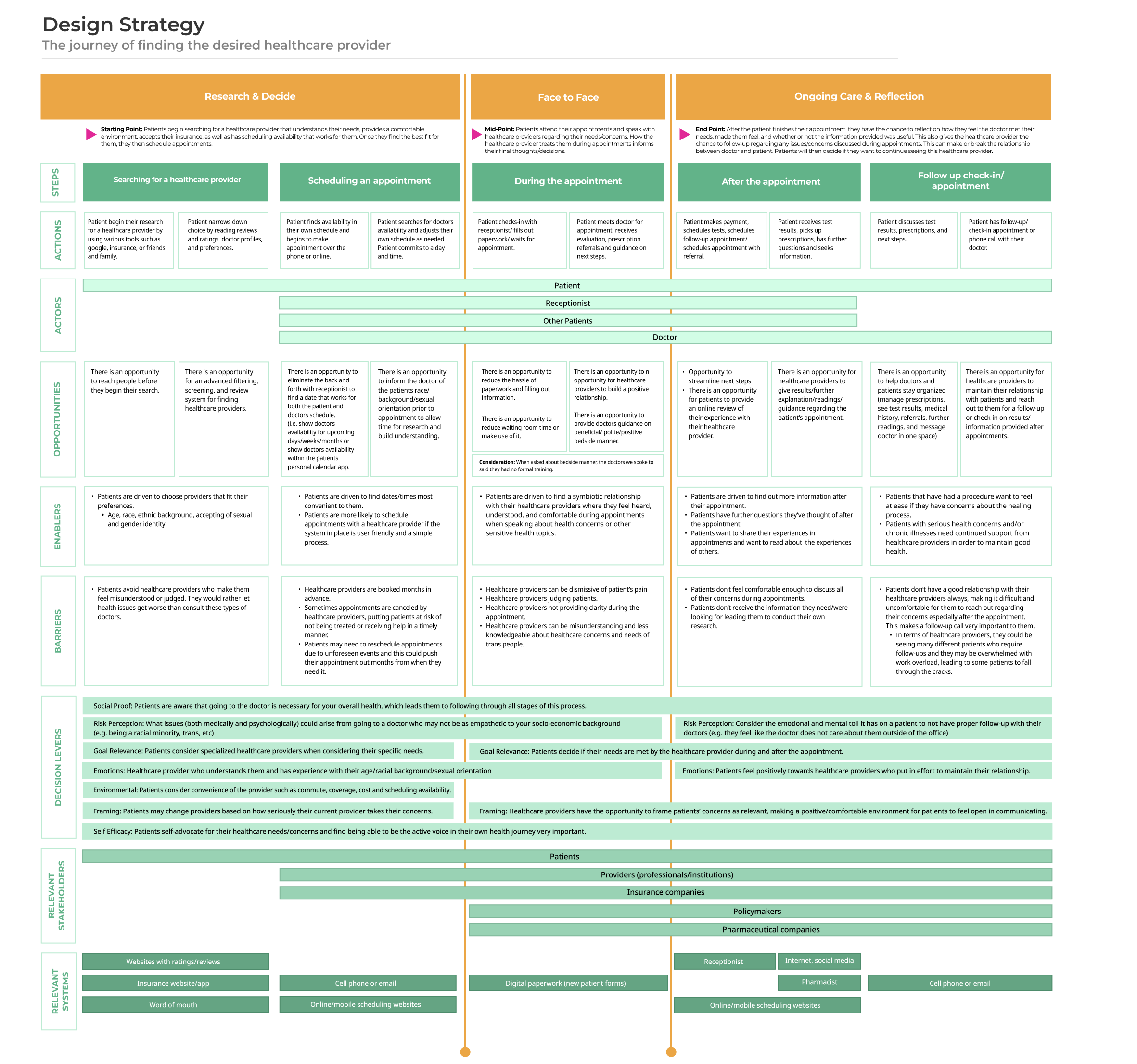
Design Strategy
The design strategy/blueprint utilized below is an expansion on the user journey map above. In this rendition, our team created broader categories for the steps outlined previously. These can be broken down into the following three stages:
- Research and Decide: searching for a healthcare provider and scheduling an appointment
- Face to Face: during the appointment
- Ongoing Care and Reflection: after the appointment and follow-up/aftercare plans
Relevant Stakeholders and Systems
Our team continued to expand on our journey map by outlining relevant stakeholders and systems necessary to meet the user's end goal. Stakeholders include patients, providers, insurance companies, policymakers, and pharmaceutical companies. Systems include ranking/review websites, insurance websites/applications, cell phones, Internet, email, online/mobile scheduling websites, digital paperwork, and social media.
Decision Levers
- Social Proof: Patients are aware that going to the doctor is necessary for your overall health, which leads them to following through all stages of this process.
- Goal Relevance: Patients consider specialized healthcare providers when considering their specific needs.
- Emotions: Healthcare providers who understand patients and have experience with their age/racial background/sexual orientation is important when choosing providers. Patients feel positively towards healthcare providers who put in effort to maintain their relationship.
- Environmental: Patients consider convenience of the provider such as commute, coverage, cost and scheduling availability.
- Self Efficacy: Patients self-advocate for their healthcare needs/concerns and find being able to be the active voice in their own health journey very important.
- Framing: Patients may change providers based on how seriously their current provider takes their concerns. Healthcare providers have the opportunity to frame patients’ concerns as relevant, making a positive/comfortable environment for patients to feel open in communicating.
- Risk Perception: What issues (both medically and psychologically) could arise from going to a doctor who may not be as empathetic to your socio-economic background (e.g. being a racial minority, trans, etc). Consider the emotional and mental toll it has on a patient to not have proper follow-up with their doctors (e.g. they feel like the doctor does not care about them outside of the office).
Final Design Concept
The objective of this prototype is to allow more control and comfortability for patients when choosing a healthcare provider so they can make informed decisions regarding their health and who they choose to form relationships with to meet healthcare goals. Another objective for this prototype on the end of the healthcare providers would be to provide them with as much background information about patients as possible in order to have successful appointments and aftercare plans in place to form more trusting relationships.
The target behavior desired for this prototype is open communication between patients and healthcare providers so that all needs are met on the patient’s end and trust/understanding is provided on the healthcare provider’s end. This would ultimately forge strong/long-lasting relationships where trust and communication are at the fore-front and healthcare concerns/questions are being dealt with properly on both ends.
Low-Fidelity Prototypes
Prioritization Process
The first stage of the journey we decided to target within our design concept was the ability for patients to search and filter when looking for a healthcare provider. This allows the patient to search according to their preferences such as a provider from a specific gender or ethnic background, as well as checking insurance coverage or out of pocket costs. We prioritized this stage in the journey because many of our interviewees expressed feelings of being misunderstood by certain healthcare providers that had different backgrounds from them. They felt unheard or misunderstood and would have preferred to have more control in choosing healthcare providers from similar backgrounds.
Another stage of the journey we prioritized was the patient being able to add notes to their appointment reservation about topics/concerns they would like to discuss during their appointment, which the healthcare provider receives on their end ahead of the appointment. This gives the patient comfortability in discussing sensitive topics and ensures they do not miss anything. Additionally, this informs the healthcare provider what patients do and do not wish to talk about. In addition, the AI integrated in the app provides the healthcare provider with rich and informative reading, including common misdiagnoses and statistics related to the patient's healthcare concerns.
Lessons Learned
- Within our literary and user research, we found that gender bias in reproductive healthcare prevents women from seeking the help they need because they feel unheard or misunderstood by current providers. They also feel that they are not taken seriously in appointments creating an environment of general distrust of all healthcare providers, leading them to suffer in silence.
- This project consisted mainly of literary and user research with little emphasis on prototyping. The final design was a low-fidelity prototype, and we did not conduct any usability testing after finalizing our concept. It would have been very interesting to see how this performed with users and if it was a useful tool.
- We conducted one-on-one interviews with participants regarding their experiences with reproductive healthcare appointments and their relationships with providers. Even though we asked about general themes of their experiences and not to explicitly describe what went on during appointments in detail, some participants may have felt obligated to share sensitive information that they otherwise would not feel comfortable expressing.
- Due to recruiting and time constraints, a missing piece of our research was the ability to interview providers themselves. This would have helped express the needs and experiences that doctors have with their patients and would have been helpful to design the Provider Portal end of our prototype.
Next Steps
- The next step in this process would be conducting user research on our low-fidelity prototype and using those results to implement a mid-fidelity prototype.
- Additionally, conducting usability testing on the mid-fidelity prototype would be necessary to improve upon this iteration further.
- Within additional rounds of user interviewing and testing of our prototype, we would like to explore the provider experience as well as the patient by adding a balanced amount of participants from each group.
- After using findings and recommendations from users to make design revisions, a final high fidelity prototype would be created.
- Using our finalized design concept, the beginning stages of development could then be conducted.